The optimal timing for non-culprit percutaneous coronary intervention in patients with multivessel coronary artery disease: A Pairwise and Network Meta-Analysis of Randomized Trials
 Network Plot
Network PlotAbstract
Background and aims: Recently, several randomized trials have shown
that patients with multivessel disease (MVD) often pursue complete
revascularization during percutaneous coronary intervention (PCI) to
improve their prognosis. However, the optimal time for the non-culprit artery
has been controversial. This study aimed to determine the optimal strategy
for revascularization in ST-segment elevation myocardial infarction (STEMI)
patients with multivessel coronary artery disease (CAD).
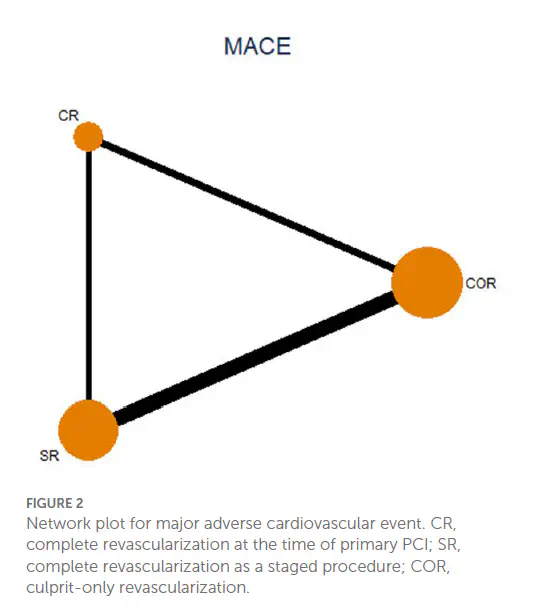
Methods: Randomized controlled trials (RCTs) comparing three
revascularization strategies [i.e., complete revascularization at the index
procedure (CR), complete revascularization as a staged procedure (SR),
or culprit-only revascularization (COR)] in STEMI patients with multivessel
coronary artery disease were included. We performed both pairwise and
network meta-analyses. Network meta-analysis was performed using mixed
treatment comparison models.
Results: 17 trials with 8568 patients were included. In the network meta-
analysis, the most interesting finding was that staged revascularization
increased the risk of major adverse cardiac events (MACE) compared with
complete revascularization at the index procedure [odds ratio (OR): 1.93;
95% confidence interval (CI): 1.07–3.49]. In the pairwise meta-analysis,
complete revascularization reduced the incidence of MACE [risk ratio
(RR): 0.62, 95% CI: 0.48–0.79, p < 0.001], mainly because it reduced
the probability of unplanned repeat revascularization (RR: 0.49, 95% CI:
0.33–0.75, p = 0.001). There were no significant dierences in all-
cause mortality, cardiac mortality, or nonfatal re-myocardial infarction (MI).
Frontiers
Conclusion: Our analysis suggests that complete revascularization should
be performed in STEMI patients with multivessel coronary artery disease,
and complete revascularization at the index procedure is superior to staged
revascularization in reducing the risk of MACE events.
Feng Y
Ph.D. Candidate
My current research interests include bioinformatics analysis, clinical cohort studies, clinical randomized controlled trials (RCTs), meta-analyses, latent class analyses ,and AI model base on medical imaging related to cancer.
{kind=link}